Intermittent
upward patellar fixation is a condition whereby the horse’s pelvic
limb temporarily "locks" in extension. As a result, there is a
delay in flexion of the limb. The delay in flexion can range from milli-seconds
to over several minutes. A short delay in flexion may manifest only as a
subtle pelvic limb asymmetry or lameness; severely affected horses (with
a long delay in flexion) may be unable to flex the affected limb without
assistance.
What
is the "Patella"?
The horse’s stifle joint is analogous to the human knee. Just like
humans, horses have a patella, or "knee cap", which slides
along the distal aspect of the femur (thigh bone) during flexion of the
joint. The patella slides within a groove (called the trochlear groove)
and serves as a fulcrum for the extensor muscles and their tendons as
they course over the front of the stifle (or knee) joint. The patella is
attached proximally to the quadriceps and biceps femoris muscles and
distally to the tibia. In humans, the patella is attached to the tibia
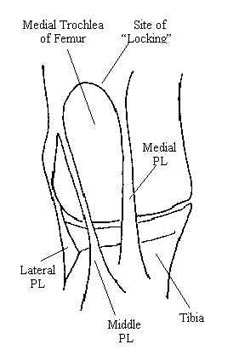
by one distal patellar ligament. Horses have 3 distal patellar
ligaments: the medial patellar ligament, the middle patellar ligament,
and the lateral patellar ligament.
How
does the horse ‘lock’ the pelvic limb? Horses
have the ability to lock (or fixate) the pelvic limb in extension. This
is possible due to the unique anatomy associated with the horse’s
stifle joint. The proximal aspect of the medial femoral trochlea is
shaped similar to a hook or ski jump. By placing the space between the
medial and middle patellar ligaments over this hook, horses can
"lock" their pelvic limbs in extension. Once locked, minimal
effort is required to maintain limb extension. A similar locking
apparatus in the thoracic limbs allows horses to sleep while
standing. Therefore, patellar fixation while standing is a normal
process in the horse.
What
is ‘intermittent upward patellar fixation’? Although
patellar fixation is normal in the standing horse, it can produce pelvic
limb dysfunction if it occurs during exercise. Inadvertent locking of
the patella over the medial femoral trochlea prevents normal flexion of
the affected limb(s). Consequently, pelvic limb asymmetry and lameness
frequently become evident.
What
causes upward patellar fixation?
There are 3 primary causes of upward patellar fixation in the horse:
- Lack
of fitness: Lack of quadriceps and/or biceps femoris muscle tone
results in an inability to quickly pull the patella up and off of
the medial femoral trochlea.
- Straight
or upright pelvic limb conformation: This places the medial femoral
trochlea further distad in closer proximity with the patella,
facilitating patellar fixation.
- Excessive
distal patellar ligament length: This places the patella proximad in
closer proximity with the medial femoral trochlea, where it can
inadvertently "catch" or "lock"
It
should be noted that the factors which cause upward patellar fixation
are often interrelated. For example, an unfit horse will generally have
increased laxity (and therefore increased length) of the distal patellar
ligaments. Furthermore, if unfitness is secondary to another disease
process (such as neurologic disease), intermittent upward fixation may
also occur secondarily. Therefore, it is important to assess the horse
as a whole prior to determining the cause for upward patellar fixation.
What
are the clinical signs?
Horses with intermittent upward patellar fixation will exhibit
clinical signs during their attempt to flex the pelvic limb from an
extended position. In acute severe cases, the pelvic limb may stay
locked in extension. The horse may not be able to flex the stifle and
tarsus without assistance. In some instances, the condition may
temporarily resolve only to recur after taking a few steps. These signs
are quite obvious and diagnosis is relatively simple if the condition is
severe. Most of the time, however, there is only a "catching"
of the patella as it slides up and over the hook and the limb does not
truly lock in extension. In this situation, there may only be a mild
pelvic limb asymmetry or lameness. This type of lameness can be easily
confused with other problems and therefore may present a dilemma in
regard to accurate diagnosis. Following are common clinical signs
associated with mild to moderate forms of intermittent upward patellar
fixation:
- Non-weightbearing
pelvic limb lameness
- This
may be distinguished from tarsal (hock) soreness which is
usually weightbearing in nature
- The
horse will frequently drag the toe of the affected limb(s)
during exercise
- Visible
wearing of the dorsal aspect of the toe/shoe may be
apparent.
- The
foot of the affected limb(s) will have a low-arc flight pattern
- The
horse will usually exhibit a shortened cranial phase to the
stride
- Resistance
in the canter
- The
horse will resist the canter, particularly if circled toward the
more affected limb
- Resistance
may be most noticeable during the transition between the trot
and canter, when the horse is forced to extend the pelvic limb
for a prolonged period
- Many
horses will toss their head, rear, or stop when asked to canter.
This may be due to their "anticipation" of impending
upward patellar fixation.
- The
horse would rather trot than canter (which is harder for the
normal horse)
- Consistent
lead changes or cantering on the wrong lead
- The
horse avoids prolonged pelvic limb extension with the affected
limb. This is particularly apparent when cantering in a circle
towards the affected limb.
- The
canter is very rough or "bouncy"
- This
occurs as a result of consistent delay in pelvic limb flexion
from the extended position
- Swelling,
heat, and/or pain may be associated with one or both stifle joints
- Upward
patellar fixation causes patellar instability which in turn may
result in femoropatellar synovitis
- The
horse drags his hind toes during exercise
- Resistance
and/or difficulty when walking up and down hills, or when backing up
- These
situations force the horse to extend the pelvic limb for a
prolonged period
- Rather
then fully extend the pelvic limb(s), the horse may
"crouch" while walking
- Rather
than flex the pelvic limb(s) normally, horses will often swing
their limbs to the outside
- This
may cause the lameness to be confused with neurologic disease
(such as EPM or stringhalt)
- Lameness
is most severe when the horse is first taken out of the stall
- Many
horses will improve as the workout progresses
- Lameness
becomes more obvious following an extended period of stall rest
- Loss
of muscle and patellar ligament tone exacerbate the upward
patellar fixation
- The
horse does not improve (and may worsen) as a result of taking
time off
- The
horse does not respond to anti-inflammatory (e.g. Phenylbutazone)
therapy
- Intermittent
upward patellar fixation is a mechanical problem and is not
inflammatory-mediated
As
with many cases of pelvic limb lameness, secondary abnormalities such as
thoracolumbar ebaxial (back) and proximal thoracic suspensory ligament
soreness are also present. These are generally detected during the
passive lameness evaluation and are suggestive of chronic pelvic limb
asymmetry/ lameness.
How
is upward patellar fixation diagnosed?
Clinical signs are characteristic and, if the limb is locked in
extension (i.e. the case is severe), diagnosis is simple. As previously
mentioned, however, most cases are mild and diagnosis may be more
difficult. A detailed history and careful clinical evaluation are
essential parts of a proper workup. One helpful diagnostic aid involves
placing the horse in one or more situations where prolonged pelvic limb
extension is normally required. Such situations include walking up and
down hills, the trot-to-canter transition, and backing up. When
confronted with these situations, the affected horse will either 1)
demonstrate upward patellar fixation by temporarily locking the pelvic
limb, or 2) cheat by switching leads, swinging the limbs to the outside,
avoiding pelvic limb extension, etc.
Many
times, a slight hitch or "catch" is visible as the pelvic limb
begins to flex from an extended position. This "catch" is most
easily detected by visualizing the point of the hock as the horse picks
the limb up to advance it cranially. Infrequently, an audible
"snap" or popping sound is also evident during exercise
(particularly walking).
In
many instances, upward patellar fixation can be produced in affected
horses by manually forcing the patella upward and outward. The examiner
may actually be able to keep the pelvic limb locked in extension using
minimal effort.
Since
the problem is usually secondary to conformation and/or level of
fitness, it is almost always bilateral. However, affected horses
historically exhibit clinical signs in one pelvic limb. It is not until
the more affected limb is successfully treated that a problem in the
contralateral limb is manifested.
How
is upward patellar fixation treated?
Currently, there are 5 forms of treatment for intermittent upward
patellar fixation:
- Exercise:
Lack of fitness results in decreased thigh muscle and patellar
ligament tone. With decreased supporting muscle and ligament tone,
it becomes easier for the patella to lock on the femur and harder
for it to replace within the trochlear groove. In subtle cases of
upward patellar fixation where conformation is relatively good,
increased exercise alone may result in resolution of the problem.
We frequently ask the client to grade the level of their horse’s
current level of fitness on a scale of 1 to 10 (1=very unfit;
10=extremely fit). We suggest achieving a fitness level of at least
7-8 (if possible) prior to pursuing other forms of treatment. This
will rule out unfitness as a major contributor to the problem as
well as increase the effect of other therapy.
- Corrective
Shoeing: Since fixation of the patella occurs when the pelvic
limb is extended, prolonging the extension phase of the stride can
make "unlocking" more difficult. Alternatively, shortening
the amount of time the pelvic limb spends in extension allows the
horse to unlock his/her patella before the distal patellar ligaments
become excessively tight. Since the conformation of the distal
pelvic limb and/or the toe length is intimately related to pelvic
limb breakover, the farrier can frequently alleviate the problem via
corrective trimming/shoeing. Rolling and/or rockering the toe of the
shoe, applying a full (egg-) bar shoe, and/or the use of wedged pads
(when needed) are commonly used techniques. In many cases, we are
able to help the pelvic limbs break over before intermittent upward
patellar fixation occurs.
- Hormonal
Therapy: The administration of estrogen has shown to prove
benefical for some horses exhibiting intermittent upward patellar
fixation. The presence of estrogen within the body of the horse may
increase tension of various supporting ligaments. These include the
collateral, suspensory, cruciate, and distal patellar ligaments.
Increasing distal patellar ligament tension helps to relocate the
patellar further distad, thereby making upward patellar fixation
more difficult. This in turn may alleviate clinical signs.
- It
should be noted that estrogen is also a powerful behavior
modificator in the horse. It is often used for stallions and
geldings that are excessively difficult to handle, aggressive
towards people or other horses, or overly anxious at shows and other
events. Estrogen is very effective at reducing anxiety and
resistance as well as improving overall behavior in these horses.
Treatment usually consists of 2 injections of estrogen (25mg) in the
muscle twice weekly for 4 consecutive weeks, then as needed
therafter.
Administration of estrogen to mares usually causes them to exhibit
clinical signs of estrus (heat). Since this change in behavior is
generally undesirable, we do not recommend its use in mares.
- Intraligamentous
Infusion of Counterirritant: This form of therapy is usually
referred to as "blistering". Blistering involves the
inject of an irritative substance into soft tissue(s) in an attempt
to create an inflammatory reaction. The irritative substance usually
consists of iodine 2% in an almond oil base. This substance can
elicit an inflammatory response for up to 30 days depending on the
amount used and the location of injection. It is important to
remember that fibrosis and scar tissue formation within normal soft
tissues will occur as a result of severe inflammation. As you know,
scar tissue does not function like normal soft tissue. Therefore,
blistering in certain areas may inhibit proper function of
associated soft tissue. It is for this reason that The Atlanta
Equine Clinic typically does not institute blistering as typical
form of treatment for soft tissue problems.
However, in the case of intermittent upward patellar fixation, we
gain a biomechanical advantage by replacing normal tissue with scar
tissue. The infusion of counterirritant within and around the medial
and middle patellar ligaments results in the elicitation of an
intense inflammatory reaction by the horse’s body. With
inflammation, fibrosis and scarring of the patellar ligaments occur.
During the scarring process, soft tissues will contract (shorten).
As the patellar ligaments shorten, the patella is pulled up and over
the hook of the medial femoral trochlea and into its normal position
within the trochlear groove. At this point, it becomes more
difficult for the horse to lock the patella and easier to flex the
pelvic limb from an extended position. In our hands, this from of
treatment has been extremely effective in a vast majority of cases
involving intermittent upward patellar fixation.
- Medial
Patellar Desmotomy: The medial patella ligament is one of the
key structures (along with the patella and middle patellar ligament)
that is required to lock the patella on the femur. Since the problem
represents the horse’s inability to quickly disengage the patella
from the medial femoral trochlea, surgical resection of the medial
patellar ligament results in complete resolution of the problem.
Once the medial patellar ligament is resected, upward patellar
fixation becomes impossible and the clinical signs associated with
this condition disappear. Consequently, this has become a very
popular form of treatment for horses with intermittent upward
patellar fixation.
It is extremely important to note, however, that the medial patellar
ligament also performs another function: stabilization of the
patella within the trochlear groove of the femur. Without tension
from the medial patellar ligament, the patella becomes unstable
within the femoropatellar joint. Femoropatellar synovitis and
frequently osteoarthritis result. Since the stifle is high-motion in
nature, chronic inflammation within this joint poses a significant
concern in regard to future performance soundness. Persistent
femoropatellar joint inflammation typically needs to be addressed on
a continual basis and often requires considerable maintenance
therapy. It is for this reason that The Atlanta Equine Clinic views
this form of treatment inappropriate except for the most severe of
cases that have proven refractory to the other forms of therapy.